
病院大規模再整備に伴うアスペルギルス感染予防対策環境感染誌 Vol. 33 no. 4, 2018 ―161 ― 〈報 告〉 病院大規模再整備に伴うアスペルギルス感染予防対策
Upload
theresa-barberCategory
view
240download
3
0
2
4
6
8
10
12
14
16
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
YEAR
(%)
E. coli
P. aeruginosa
*C. albicans
Yeast form fungi
K. pneumoniae
S. aureus
Enterococcus
*A. baumannii
Coag. (-) staph.
E.cloacae
*2000年開始鑑定
台北院區院內感染常見 10種致病菌歷年變化
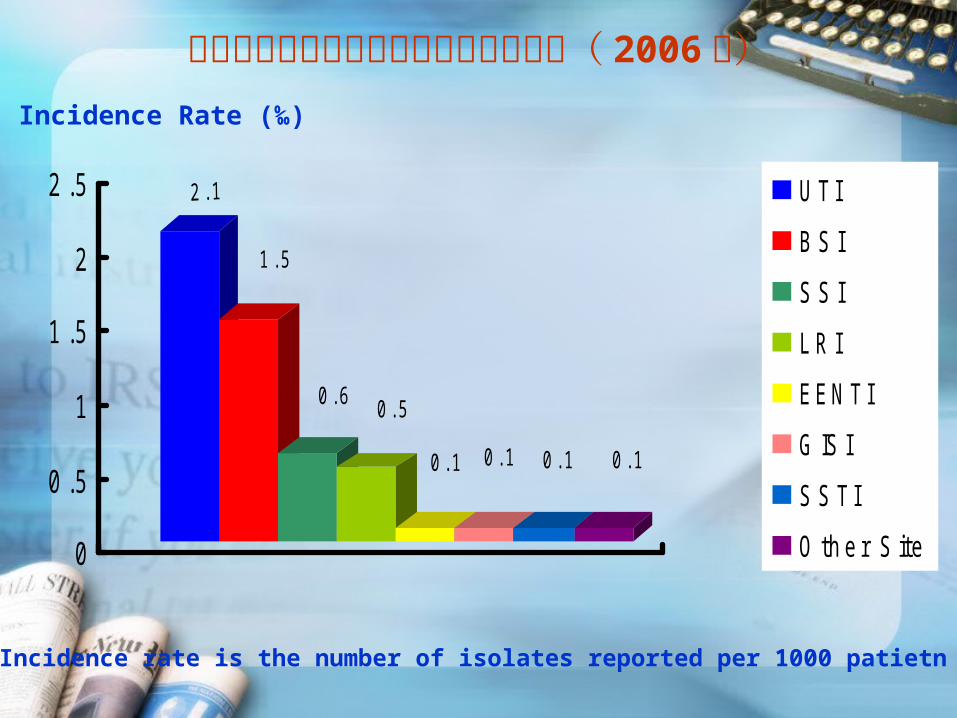
1 . 5
0 . 6 0 . 5
0 . 1 0 . 1 0 . 1 0 . 1
0
0 .5
1
1 .5
2
2 .5 U T I
B S I
S S I
L R I
E E N T I
G IS I
S S T I
O t h e r S it e
Incidence Rate (‰)
Incidence rate is the number of isolates reported per 1000 patietn days
台北院區院內感染各部位感染發生密度( 2006年)
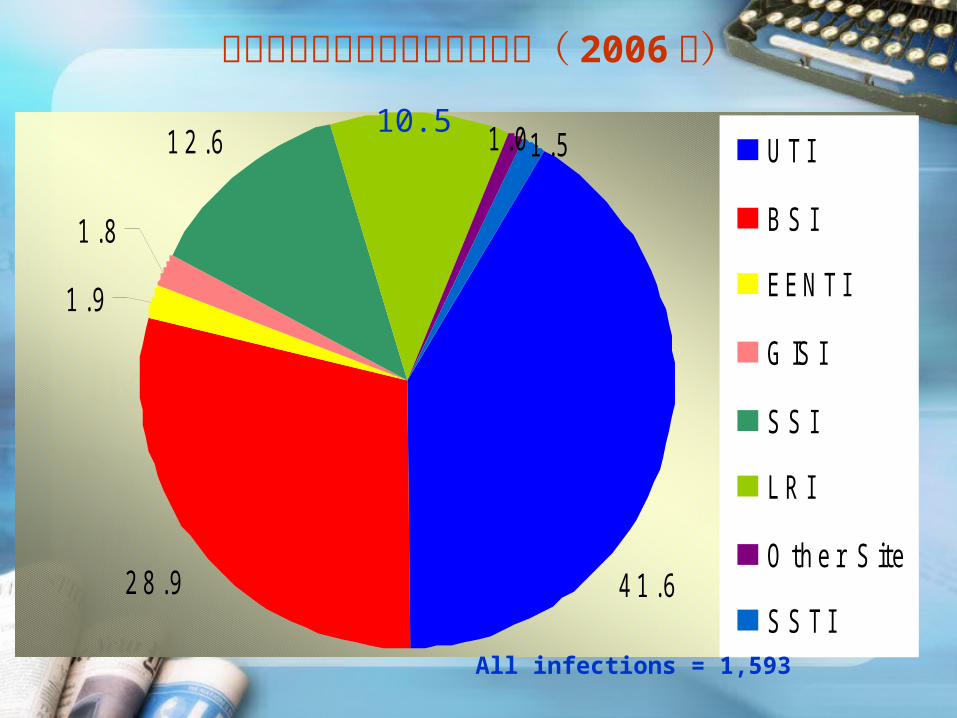
2 8 . 9
1 . 9
1 . 8
1 2 . 6
1 0 . 5
1 . 0 1 . 5
4 1 . 6
U T I
B S I
E E N T I
G IS I
S S I
L R I
O t h e r S it e
S S T I
All infections = 1,593
台北院區院內感染各部位分佈圖( 2006年)
10.5

9 . 8
9 . 6
8 . 4
8 . 4
7 . 2
6 . 9
3 . 5
2 . 1
1 1 . 9
7 .7
2 . 9
2 . 4
2 . 3
2 . 0
1 . 7
0 .0 2 .0 4 .0 6 .0 8 .0 10 .0 12 .0 14 .0
S . m a l t o p h i l i a
S . m a r c e s c e n s
P . m i r a b i l i s
O t h e r G N F b a c t e r i a
O t h e r S t r e p t o c o c c u s
E . c l o a c a e
C o a g u l a s e ( - ) S t a p h y l o c o c c u s
A . b a u m a n n i i
E n t e r o c o c c u s
S . a u r e u s
Y e a s t fo r m fu n g i
K . p n e u m o n i a e
C . a l b i c a n s
P . a e r u g i n o s a
E . c o l i
%
台北院區院內感染常見的 15種致病菌( 2006年)
Total 1,759

PATHOGEN LRI SSI GISIEENT
IBSI UTI SSTI
Others
TOTAL ISOLAT
E%
E. coli 2.5 7.8 0.0 0.0 13.4 14.2 4.5 11.1 210 11.9
P. aeruginosa 16.5 11.0 10.0 19.0 6.3 10.8 13.6 5.6 172 9.8
C. albicans 1.3 1.8 0.0 0.0 3.9 18.1 0.0 0.0 168 9.6
K. pneumoniae 0.0 2.1 5.0 4.8 8.6 11.5 9.1 11.1 148 8.4
Yeast form fungi 0.0 0.7 0.0 0.0 3.5 16.0 0.0 5.6 147 8.4
S. aureus 15.2 14.8 0.0 23.8 9.7 1.7 27.3 27.8 135 7.7
Enterococcus 1.3 9.9 0.0 4.8 5.6 8.2 4.5 5.6 126 7.2
A. baumannii 35.4 2.8 0.0 4.8 7.5 5.3 13.6 5.6 122 6.9
Coagulase(-) Staphylococcus
0.0 2.8 0.0 4.8 6.9 1.8 4.5 5.6 62 3.5
E. cloacae 0.0 4.2 0.0 0.0 5.0 1.5 0.0 0.0 51 2.9
Other Streptococcus 1.3 8.1 0.0 4.8 1.9 0.9 0.0 5.6 43 2.4
Other GNF bacteria 1.3 2.1 0.0 0.0 5.4 0.5 0.0 0.0 40 2.3
P. mirabilis 0.0 2.5 0.0 4.8 1.1 2.7 4.5 5.6 37 2.1
S. marcescens 0.0 2.1 0.0 0.0 3.2 1.5 0.0 0.0 35 2.0
S. maltophilia 10.1 0.4 0.0 0.0 2.8 0.6 4.5 0.0 30 1.7
All others 15.2 26.9 85.0 28.6 15.1 4.4 13.6 11.1 233 13.2
NUMBER OF ISOLATES
79 283 20 21 536 780 22 18 1,759 100.00
台北院區院內感染常見的 15種致病菌各部位之感染率( 2006年)

1 7 .9
1 6
1 4 .1
1 1 .4
1 0 .4
8 .1
5 .2
2 .7
1 .8
1 .7
1 .5
1 .5
1
0 .9
0 .9
5
0 5 1 0 1 5 2 0
%
A l l o th e rs
A c i n e to b a c te r s p p .
O th e r s t re p to c o c c u s
C i t ro b a c te r s p p .
S e rra t i a m a rc e s c e n s
E . c l o a c a e
S . a u re u s
C o a g u l a s e (-) s ta p h y l o c o c c u s
P ro te u s m i ra b i l i s
A c i n e to b a c te r b a u m a n n i i
E n te ro c o c c u s
P . a e ru g i n o s a
K . p n e u m o n i a e
E . c o l i
Y e a s t fo rm fu n g i
C a n d i d a a l b i c a n s
台北院區院內感染 UTI常見的致病菌( 2006年)
Total 782
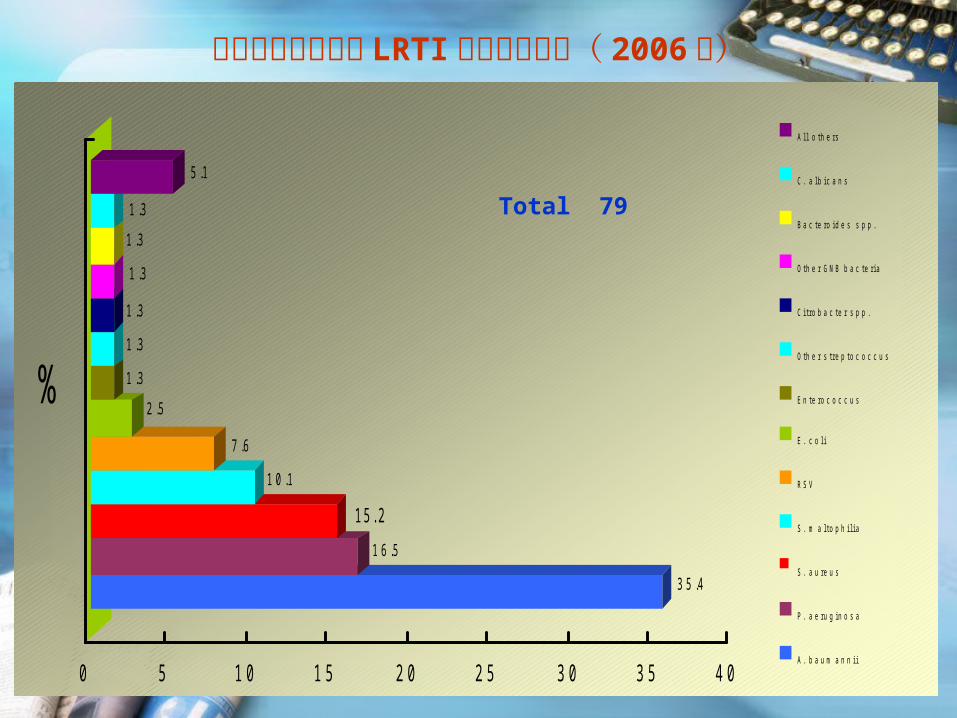
3 5 .4
1 6 .5
1 5 . 2
1 0 .1
7 .6
2 .5
1 .3
1 .3
1 .3
1 .3
1 .3
1 .3
5 .1
0 5 1 0 1 5 2 0 2 5 3 0 3 5 4 0
%
A l l o t h e r s
C . a l b i c a n s
B a c t e r o i d e s s p p .
O t h e r G N B b a c t e r i a
C i t r o b a c t e r s p p .
O t h e r s t r e p t o c o c c u s
E n t e r o c o c c u s
E . c o l i
R S V
S . m a l t o p h i l i a
S . a u r e u s
P . a e r u g i n o s a
A . b a u m a n n i i
台北院區院內感染 LRTI常見的致病菌( 2006年)
Total 79

1 4 .9
1 0 .8
9.78 .3
8
7.6
4 .5
4 .2
4 .2
2 .8
2 .8
2 .4
2.4
2.12 .1
1 3 .2
0 5 10 15
%
A l l o t h e r s
S . m a r c e s c e n s
K . p n e u m o n i a e
O t h e r G N F b a c t e r i a
P r o t e u s m i r a b i l i s
A c i n e t o b a c t e r b a u m a n n i i
C o a g u l a s e ( - ) s t a p h y l o c o c c u s
A n a e r o b i c G ( + ) c o c c i
E . c l o a c a e
F u s o b a c t e r i u m s p p .
E . c o l i
B a c t e r o i d e s f r a g i l i s
O t h e r s t r e p t o c o c c u s
E n t e r o c o c c u s
P . a e r u g i n o s a
S . a u r e u s
台北院區院內感染 SSI常見的致病菌( 2006年)
Total 288

1 3 .4
9 .7
8 .9
7 .4
6 .9
6 .3
5 .6
5 .453 .9
3 .5
3 .2
2 .8
2 .8
2
1 3 .2
0 5 10 15
%
A l l o th e rs
O th e r s t re p to c o c c u s
S . m a l t i o h i l i a
A c i n e to b a c te r s p p .
S . m a rc e s c e n s
Y e a s t f o rm f u n g i
C . a l b i c a n s
E . c l o a c a e
O th e r G N F b a c te r i a
E n te ro c o c c u s
P . a e ru g i n o s a
C o a g u l a s e ( - ) s ta p h y l o c o c c u s
A . b a u m a n n i i
K . p n e u m o n i a e
S . a u re u s
E . c o l i
台北院區院內感染 BSI常見的致病菌( 2006年)
Total 538

4 0
1 2
1 2
8
8
4
4
4
4
4
0 10 2 0 3 0 4 0
%
C . a l b i c a n s
S . m a l to p h i l i a
E . c o l i
G ro u p A s t re p to c o c c u s
E n te ro c o c c u s
B a c te ro i d e s f ra g i l i s
K . p n e u m o n i a e
A . b a u m a n n i i
P . a e ru g i n o s a
S . a u re u s
台北院區院內感染 SSTI常見的 15種致病菌( 2006年)
Total 25
What organisms are most likely?
何種致病菌是最可能造成此次感染的致病菌 ?
適當的經驗療法臨床症候群 (Clinical syndrome)
宿主因素 (Host factor)
流行病學資料 (Epidemiological data)

If several antibiotics are available, which is best?
(This question involves such factors as drugs of choice, pharmacokinetics, toxicology, cost, narrowness of spectrum, and bactericidal compared with bacteriostatic agents.)
對於一個最可能的致病菌,或是已確定的致病菌,可能有多種藥物可用來治療,何者才是最佳的選擇藥物 ?
Staphylococcus aureus: Antibiotics Methocillin-sensitive S. aureus (MSSA): 首選藥物 : oxacillin 替代藥物 : 第一代頭孢菌素 假如 penicillin allergic - Erythromycin, Clinda
mycin, Glycopeptide (Vancomycin, Teicoplanin)
Methocillin-resistant S. aureus (MRSA) : 首選藥物 :Glycopeptide (Vancomycin, Teicopl
anin) 替代藥物 : Linezolid Fusidic acid Rifampicin
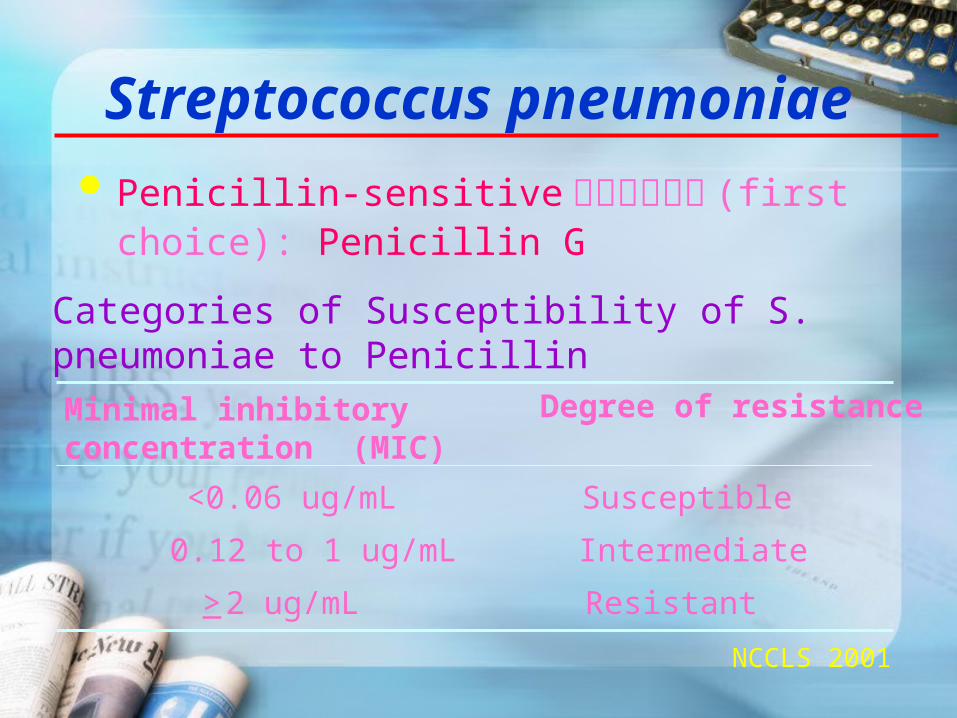
Categories of Susceptibility of S. pneumoniae to Penicillin
NCCLS 2001
Minimal inhibitory concentration (MIC)
Degree of resistance
<0.06 ug/mL Susceptible
0.12 to 1 ug/mL Intermediate
> 2 ug/mL Resistant
Streptococcus pneumoniae
Penicillin-sensitive 菌株首選藥物 (first choice): Penicillin G
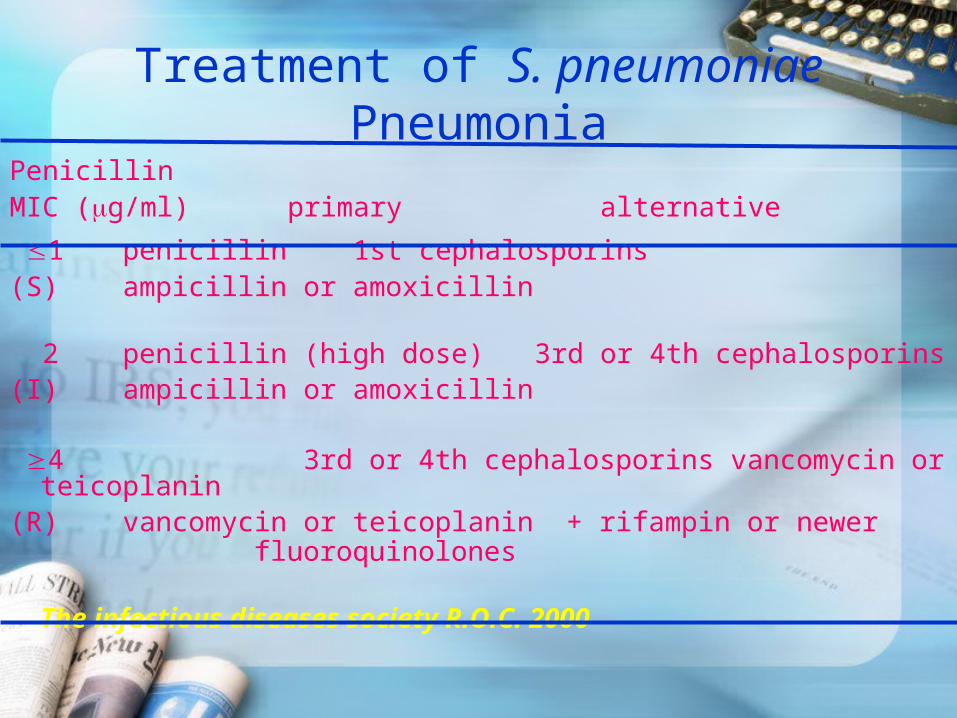
Treatment of S. pneumoniae Pneumonia
Penicillin MIC (g/ml) primary alternative
1 penicillin 1st cephalosporins(S) ampicillin or amoxicillin 2 penicillin (high dose) 3rd or 4th cephalosporins(I) ampicillin or amoxicillin
4 3rd or 4th cephalosporins vancomycin or teicoplanin(R) vancomycin or teicoplanin + rifampin or newer
fluoroquinolones
The infectious diseases society R.O.C. 2000
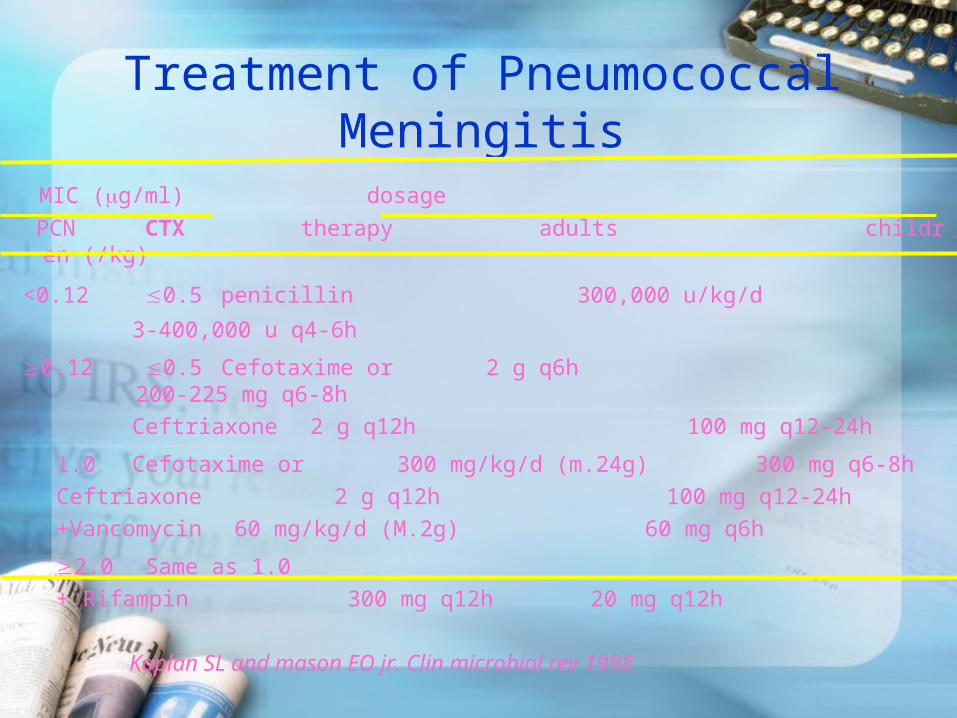
Treatment of Pneumococcal Meningitis
MIC (g/ml) dosage
PCN CTX therapy adults children (/kg)
<0.12 0.5 penicillin 300,000 u/kg/d 3-400,000 u q4-6h
0.12 0.5 Cefotaxime or 2 g q6h 200-225 mg q6-8h
Ceftriaxone 2 g q12h 100 mg q12-24h
1.0 Cefotaxime or 300 mg/kg/d (m.24g) 300 mg q6-8h
Ceftriaxone 2 g q12h 100 mg q12-24h
+Vancomycin 60 mg/kg/d (M.2g) 60 mg q6h
2.0 Same as 1.0
+ Rifampin 300 mg q12h 20 mg q12h
Kaplan SL and mason EO jr. Clin microbiol rev 1998

Streptococcus pneumoniae依 CNS Infection 和 Non- CNS Infection (P
neumonia, bacteremia) 不同部位感染,按照 MIC 值選擇藥物治療。
Invasive Pneumococcal disease 經驗治療 Non- CNS Infection (Pneumonia, bacteremia): hig
h dose penicillin G, or other cephalosporins (ceftriaxone;cefotaxime),or newer fluoroquinolones. Not vancomycin 。
CNS Infection (Meningitis): Not Penicillin, vancomycin + ceftriaxone (cefotaxime, Cefepime, Cefpirome, Meropenem)
Enterococci sp.
E. faecalis, E. faecium
Habitat: commensal of human and animal gut
Lancefield group D, bile resistant
Infections
- Urinary tract infection
- Intra-abdominal sepsis
- Biliary tract infection
- Endocarditis

Enterococci sp. 首選藥物 : Ampicillin
心內膜炎加上 gentamicin 有加成作用 (synergistic effect)
Never use cephalosporins or aminoglycosides alone or Clindamycin, TMP/SMX for Enterococci
對 ampicillin 抗藥性 : Glycopeptide
Vancomycin-resistant Enterococci(VRE) -
Quinupristin/dalfopristin
Linezoid
Chloramphenicol
Klebsiella pneumoniae 首選藥物 (first choice): cephalosporins
無併發症感染 : cefazolin + aminoglycosides
嚴重感染合併眼內炎、腦膜炎 : third generation ce
phalosporins 為首選藥物 不建議使用 penicillins 類藥物 (Unasyn, augmentin,
Timentin, tazocin 均不建議使用 )

Escherichia coli
Most common possible etiologies:
1. Cystitis & pyelonephritis
2. Emphysematous pyelonephritis.(DM)
3. Acute bacterial prostatitis
首選藥物 (first choice):
-lactam antibiotics + aminoglycosides 。 台灣地區第一線可用 cefazolin , 80% 對 ampicillin 抗藥性。
Klebsiella sp. & Escherichia coli
In vitro resistant to any of the third generation cephalosporins
Strain produced an extended-spectrum -lactamases (ESBL)
Resistance to all penicillins, cephalosporins & aztreonam
首選藥物 (first choice): Carbapenem Cephamycins (AmpC -lactamases) Piperacillin-tazobactam(Tazocin) ( AmpC -lactamases) Ciprofloxacin
Aminoglycosides

Citrobacter, Enterobacter, Acinetobacter, Serratia, Providencia Species
Hospital acquired pathogens: UTI, ventilator associated pneumonia, septicaemia
Antibiotic susceptibility unpredictable since often multiply antibiotic resistant; need susceptibility test guidance of treatment
Inducible ß- lactamase(Amp C)
4th cephalosporin(Maxipime, Cefrom), Imipenem-cilastatin, Meropenem
Pseudomonas aeruginosaHabitat: GIT of humans & animals, environmentWater; survives in hospitals (In antiseptics)Obligate aerobe, gram-negative rods, polar flagella, oxidase positive (in contrast to Enterobacteriaceae)Infections:Hospital acquired infections: UTI with urinary catheter, pneumonia (cystic fibrosis, ventilator associated), burns infection, septicaemia in immunocompromised (transplantation, oncology, ICU)Chronic otitis media & externaEye infection secondary to trauma
Pseudomonas aeruginosaAntipseudomonal Antibiotics: Ceftazidime(Fortum)
Cefepime(Maxipime), Cefpirome(Cefrom)
Aztreonam
Imipenem-cilastatin / Meropenem
Piperacillin, Piperacillin-tazobactam(Tazocin)
Ticarcillin, Ticarcillin-clavulanate(Timentin)
Ciprofloxacin, Levofloxacin
Aminoglycosides
Acinetobacter baumannii
造成嚴重院內感染之革蘭氏染色陰性菌之一 首選藥物 (first choice): Imipenem/Cilastatin (Ti
enam®) / Meropenem
替代藥物 : Ampicillin/sulbactam (Unasyn® ) o
r sulbactam, Colistin, Tigecycline (Tygacil® )

Stenotrophomonas maltophilia
造成嚴重院內感染之革蘭氏染色陰性菌之一
首選藥物 (first choice): TMP/SMX ; Co-trimoxazole
替代藥物
1. Moxalactam
2. Timentin (Ticarcillin-clavulanate)
3. Ciprofloxacin, Levofloxacin

Is an antibiotic combination appropriate?
是否需要合併使用兩種或以上的抗生素 ?
Febrile leukopenic patient
In infections in which multiple organisms are likely or proved
Synergism
Serial inhibition of microbial growth
One antibiotic enhances the penetration of another
Limiting or preventing the emergence of resistance

Combination TherapyTuberculosisDisseminated Mycobacterium avium complexHelicobacter pyloriEndocarditis(alpha haemolytic streptococcus, enterococcal )
• Vancomycin-resistant enterococcal disease
• Life-threatening infection caused by P. aeruginosa
• Empiric treatment ( pneumococcal meningitis; febrile, severely neutropenic host; polymicrobic infection; life-threatening infection with inapparent source)

Gentamicin加上 Gentamicin 有加成作用 (Synergistic effect) Enterococci endocarditis( 心內膜炎 ) or bactere
mia Gentamicin + Ampicillin or penicillin G Viridans streptococci endocarditis: Gentamicin + penicillin G MRSA or S. epidermidis : prosthetic valve endo
carditis Vancomycin+ GentamicinListeria mononcytogenes: Ampicillin + Gentamic
inSerious Pseudomonas aeruginosa infection Ami
noglycosides + Anti-Pseudomonal agents

The use of monotherapy with antipseudomonal penicillins or cephalopsorins for patient with severe P. aeruginosa infections can lead to the emergency of antimicrobial-resistant strain.
Combination of 2 antipseudomonal ß - lactam antibiotics lacks synergy in animal models & in human
Combination of an aminoglycosides & antipseudomonal ß - lactam antibiotics works synergistically against P. aeruginosa & improved clinical outcome.
Pseudomonas aeruginosa
Todd FH et al CID 2000; 31:1349-56
AMERICAN THORACIC SOCIETY DOCUMENTS:
Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Heal
thcare-associated Pneumonia
Am. J. Respir. Crit. Care Med. 2005; 171: 388-416

Executive Summary
Introduction
Methodology Used to Prepare the Guideline
Epidemiology
Incidence
Etiology
Major Epidemiologic Points
Pathogenesis
Major Points for Pathogenesis
Modifiable Risk Factors
Intubation and Mechanical Ventilation
Aspiration, Body Position, and Enteral Feeding
Modulation of Colonization: Oral Antiseptics and Antibiotics
Stress Bleeding Prophylaxis, Transfusion, and Glucose Control
Major Points and Recommendations for Modifiable Risk Factors
Diagnostic Testing
Major Points and Recommendations for Diagnosis
Diagnostic Strategies and Approaches
Clinical Strategy
Bacteriologic Strategy
Recommended Diagnostic Strategy
Major Points and Recommendations for Comparing Diagnostic Strategies
Antibiotic Treatment of Hospital-acquired Pneumonia
General Approach
Initial Empiric Antibiotic Therapy
Appropriate Antibiotic Selection and Adequate Dosing
Local Instillation and Aerosolized Antibiotics
Combination versus Monotherapy
Duration of Therapy
Major Points and Recommendations for Optimal
Antibiotic Therapy
Specific Antibiotic Regimens
Antibiotic Heterogeneity and Antibiotic Cycling
Response to Therapy
Modification of Empiric Antibiotic Regimens
Defining the Normal Pattern of Resolution
Reasons for Deterioration or Nonresolution
Evaluation of the Nonresponding Patient
Major Points and Recommendations for Assessing Response to Therapy
Suggested Performance Indicators
Contents
Executive Summary(1)Official statement of ATS/IDSA, evidence-based
HCAP: included in the spectrum of HAP/VAP, need therapy of MDR pathogen
Lower resp. tract cultures (LRTCs): quantitative (specificity of diagnosis) or semi-quantitative; non- or bronchoscopical collection for all cases
Negative LRTCs: may stop ABx without ABx changes in the past 72 hrs
Executive Summary(2)Early, appropriate, broad-spectrum, antibiotic therapy with adequate doses to optimize antimicrobial efficacyEmpiric regimen should include with a different
antibiotic class agents than those recently receivedCombination therapy for a specific pathogen Consideration of short-duration (5 days) aminogl
ycoside, when used in combination with a β-lactam to treat P. aeruginosa pneumonia

Executive Summary(3)Linezolid: an alternative to vancomycin; may have an advantage for proven VAP due to MRSA (unconfirmed, preliminary data) Colistin: considered in VAP due to a carbapenem-resistant Acinetobacter speciesAerosolized antibiotics: may have value as adjunctive therapy in VAP due to some MDR pathogensDe-escalation of ABx: should be considered once; according to the results of LRTCs and the patient’s clinical response
Executive Summary(4)A shorter duration of ABx therapy (7 to 8 days): r
ecommended for - uncomplicated HAP, VAP, or HCAP - with initially appropriate therapy - a good clinical response - with no evidence of infection with non- fermenting gram-negative bacilli
Introduction(1)HAP: pneumonia occurs 48 hrs after admission ( not intubated at admission)VAP: pneumonia occurs48-72 hrs after intubationHCAP: pneumonia occurs including those
- hospitalized in an acute care hospital for 2 days within 90 days - received recent IV antibiotic therapy, chemotherapy, or wound care within the past 30 days - resided in a nursing home or long-term care facility - attended a hospital or hemodialysis clinic

Introduction(2)4 major principles to manage HAP, VAP, HCAP:
Avoid untreated or inadequately treatment; because failure to initiate prompt appropriate and adequate therapy increased mortality
Avoid the overuse of antibiotics by focusing on accurate diagnosis, tailoring therapy to the results of LRTCs, and shortening duration of therapy to the minimal effective period

Introduction(2)4 major principles to manage HAP, VAP, HCAP:
Recognize the variability of bacteriology from one hospital to another, specific sites within the hospital, and from one time period to another, and use this information to alter the selection of an appropriate antibiotic treatment regimen for any specific clinical setting
Apply prevention strategies aimed at modifiable risk factors
Epidemiology (1)Time of onset of pneumonia: an important epidemiologic variable and risk factor for specific pathogens and outcomes
Early-onset HAP and VAP( 4 days): usually better prognosis, more likely to be caused
by antibioticsensitive bacteria (Level II)
Epidemiology (2)Late-onset HAP and VAP ( 5 days ): usually with increased mortality and morbidity, more likely to be caused by multidrug-resistant (MDR) pathogens (Level II)
Early-onset HAP with prior ABx or prior hospitalization within the past 90 days: are at greater risk for colonization and infection with MDR pathogens treat as late-onset HAP or VAP (Level II)
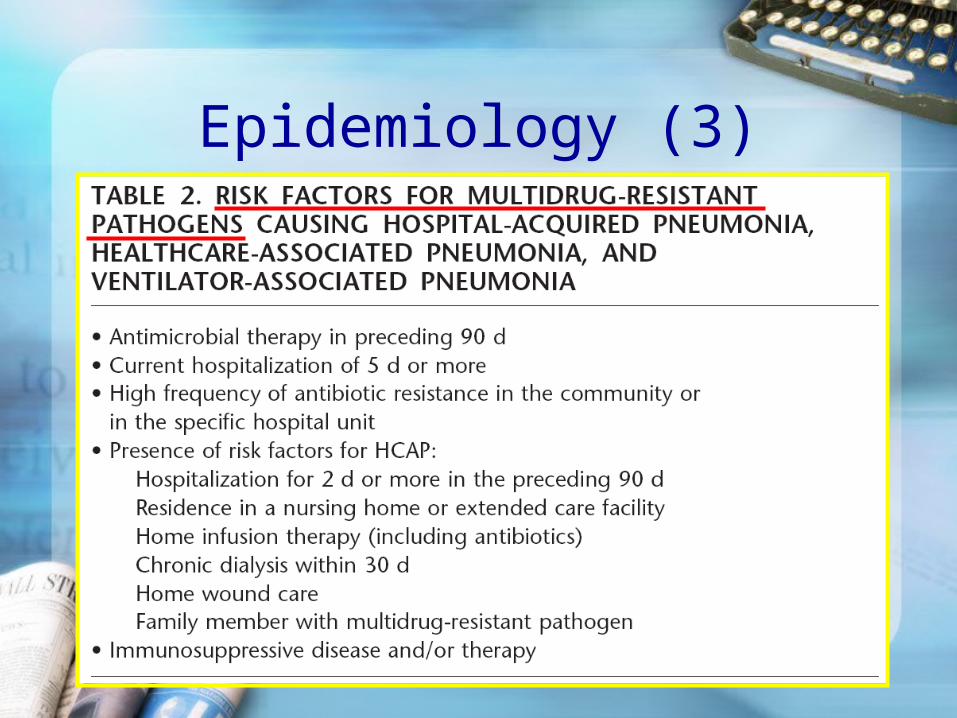
Epidemiology (3)

Epidemiology (4) HAP/VAP Pts: risk for colonization and infection
with MDR pathogens (Level II)
Incidence of HAP/VAP: difficult to define exactly (overlap with tracheobronchitis) (Level III)
The exact incidence of HAP: usually between 5~15/1,000 admissions (Level II)
The exact incidence of VAP: 6~20-fold greater than in non-ventilated patients (Level II)

Epidemiology (5)Causes of most cases of HAP, VAP, and HCAP: Bacteria, usually polymicrobial; especially high rate in patients with ARDS (Level I)
Common bacteria: (Level II) - Aerobic GNB: P. aeruginosa, K. pneumoniae, and Acinetobacter species - Aerobic GPC, such as S. aureus ( much MRSA) - Anaerobes: uncommon .
Epidemiology (6)Rates of L. pneumophila: vary between hospitals, occurs commonly in serogroup1; with colonized water supply and ongoing construction (Level II)
Nosocomial virus and fungal infections: uncommon in immunocompetent patients (Level I)
Outbreaks of influenza: occurred sporadically and risk of infection reduced with widespread effective infection control, vaccination, and use of antiinfluenza agents (Level I)

Epidemiology (7)Prevalence of MDR pathogens: varies by patient population, hospital, and type of ICU; need for local surveillance data (Level II)
MDR pathogens: (Level II)
more commonly isolated from patients - with severe, chronic underlying disease - with risk factors for HCAP - with late-onset HAP or VAP

Pathogenesis (1)Sources of pathogens: (Level II)
- healthcare devices - the environment (air, water, equipment, and fomites) - transfer of microorganisms between patients and staffs
Host- and treatment-related colonization factors: important pathogenesis: (Level II) - the severity of underlying disease - prior surgery - exposure to antibiotics - other medications - exposure to invasive respiratory devices and equipment
Pathogenesis (2)Primary routes of bacterial entry: (Level II)
- aspiration of oropharyngeal pathogens - leakage of secretions which containing bacteria around tube cuff
Uncommon pathogenic mechanisms (Level II) - inhalation or direct inoculation of pathogens - hematogenous spread from infected intravenous catheters - bacterial translocation from GI tract

Pathogenesis (3)Infected biofilm in the endotracheal tube, with subsequent embolization to distal airways, may be important in the pathogenesis of VAP (Level III)
Stomach and sinuses: potential reservoirs of pathogens, contribute to bacterial colonization of the oropharynx, but their contribution is controversial (Level II)

Modifiable Risk Factors (1)General prophylaxis.
Effective infection control measures: (Level I) -staff education -alcohol-based hand disinfection -isolation: cross-infection with MDR pathogens
Surveillance of ICU infections: (Level II) to identify and quantify endemic and new MDR
pathogens, and preparation of timely data for infection control
Modifiable Risk Factors (2)Intubation and mechanical ventilation
Avoid intubation and reintubation (risk of VAP) (Level I)
Noninvasive ventilation should be used whenever possible in selected patients (Level I)
Orotracheal intubation and orogastric tubes are preferred over nasotracheal intubation and nasogastric tubes to prevent nosocomial sinusitis and to reduce the risk of VAP ( direct causality has not been proved) (Level II)
Modifiable Risk Factors (3)Intubation and mechanical ventilation
Continuous aspiration of subglottic secretions: risk of early-onset VAP (Level I)
Cuff pressure 20 cm H2O to prevent leakage of bacterial pathogens (Level II)
Clear contaminated condensate from ventilator circuits and prevent to enter either the endotracheal tube or inline medication nebulizers (Level II)
Modifiable Risk Factors (4)Intubation and mechanical ventilation
Passive humidifiers or heat–moisture exchangers: circuit colonization, but not consistently incidence of VAP not a pneumonia prevention tool (Level I)
duration of intubation and MV: may prevent VAP, achieved by the use of sedation and to accelerate weaning (Level II)

Modifiable Risk Factors (5)Aspiration, body position, and enteral feeding.
Kept in the semirecumbent position (30–45) rather than supine to prevent aspiration, especially
when receiving enteral feeding (Level I)
Enteral nutrition: preferred over parenteral nutrition (Level I)
- risk of complications related to CVP - prevent reflux villous atrophy of intestinal mucosa ( wh
ichrisk of bacterial translocation)

Modifiable Risk Factors (6)Modulation of colonization:oral antiseptics and ABx
Routine prophylaxis of HAP with oral antibiotics with or without systemic antibiotics:
-incidence of VAP -has helped contain outbreaks of MDR bacteria (Level I) Not recommended especially in patients who may b
e colonized with MDR pathogens (Level II)
Onset of infection with prior systemic ABx suspicious infection with MDR pathogens (Level
II)

Modifiable Risk Factors (7)Modulation of colonization:oral antiseptics and ABx
Prophylactic systemic ABx for 24 hrs at the time of intubation: demonstrated to prevent HAP in patients with closed head injury, but not recommended a routine until more data become available (Level I)
Modulation of oropharyngeal colonization by the use of oral chlorhexidine: has prevented HAP in CABG, but not recommended a routine until more data become available (Level I)
Modifiable Risk Factors (8)Modulation of colonization:oral antiseptics and ABx
Use daily interruption or lightening of sedation to avoid constant heavy sedation and try to avoid paralytic agents, both of which can depress cough and thereby risk of HAP (Level II)
Modifiable Risk Factors (9)Stress bleeding prophylaxis, transfusion
Sucralfate: VAP, but slightly rate of significant gastric bleeding compared with H2 antagonists. Stress bleeding prophylaxis: H2 antagonists or sucralfate is acceptable (Level I)
Transfusion of RBC with a restricted policy; leukocyte-depleted RBC transfusions can HAP in selected patient populations (Level I)
Modifiable Risk Factors (9)Hyperglycemia
Intensive insulin therapy: recommended to maintain BS between 80 and 110 mg/dl in ICU patients
- nosocomial blood stream infections - duration of mechanical ventilation - ICU stay - morbidity - mortality (Level I)
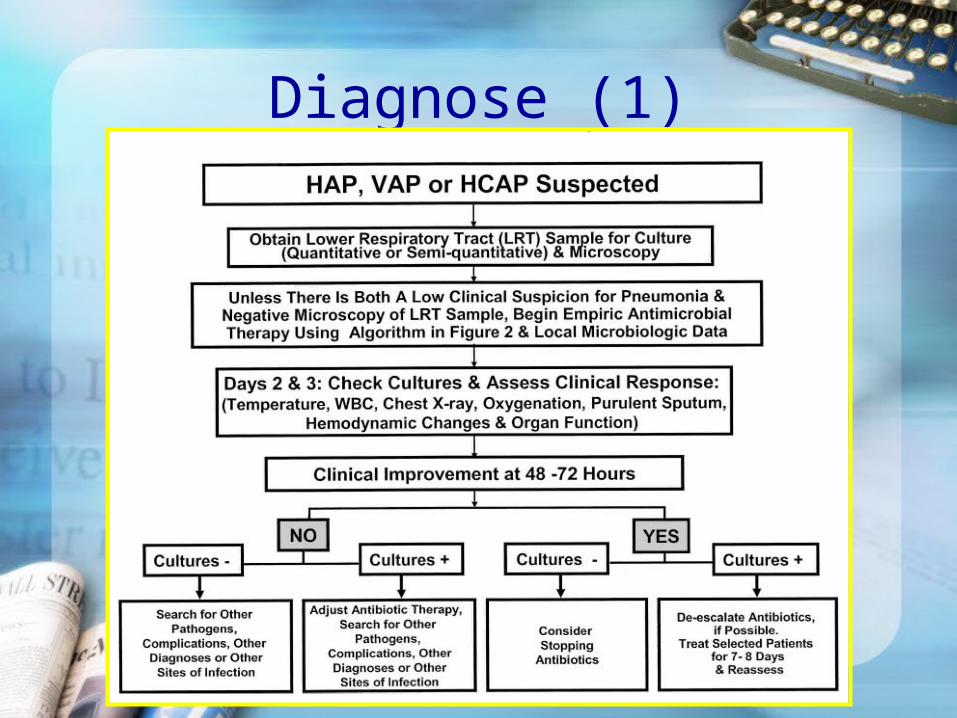
Diagnose (1)

Diagnosis (2)Ccomprehensive medical history, PE, CXR, sever
ity of HAP, exclude other potential infection, specific conditions that can influence the likely etiologic pathogens (Level II)
Tracheal colonization: does not require therapy or diagnostic evaluation in the absence of clinical findings or sign of infection (Level II)
Diagnosis (3)Blood cultures: All patients should collect; A positive result indicate pneumonia or extra-pulmonary infection (Level II)
Sample collection: Protected specimen brush sample
s- specificity>sensitivity; Endotracheal aspirate, BAL-sensitivity>specificity (Level II)
Diagnostic threshold of quantitative culture: PSB 103 cfu/ml; BAL 104~105 cfu/ml; tracheal aspirates 106 cfu/ml

Diagnosis (4)A sterile culture without a new antibiotic in the past 72 hours: virtually rules out the presence of bacterial pneumonia (NPV 94%), but viral or Legionella infection is still possible (Level II)
Semiquantitative cultures of tracheal aspirates cannot be reliably as quantitative cultures to define the presence of pneumonia and the need for antibiotic therapy (Level I)
Diagnosis (5)Bronchoscopic bacteriologic strategy: 14-day mortality, compared with a clinical strategy in VAP (Level I) should not postpone diagnostic studies in clinically unstable (Level II)

Treatment (1)

Treatment (2)

Treatment (3)
Penicillin-resistant S. pneumoniae and multidrug-resistant S. pneumoniae: frequency; levofloxacin or moxifloxacin are preferred to ciprofloxacin and the role of other new quinolones, such as gatifloxacin, has not been established

Treatment (4)•ESBL strain: such as K. pneumoniae or Acinetobacter: carbepenem is a reliable choice. • L. pneumophila: combination antibiotic regimen should include macolide (azithromycin) or a fluoroquinolone (e.g., ciprofloxacin or levofloxacin) • MRSA risk factors are present or there is a high incidence locally: Vancomycin or linezolid
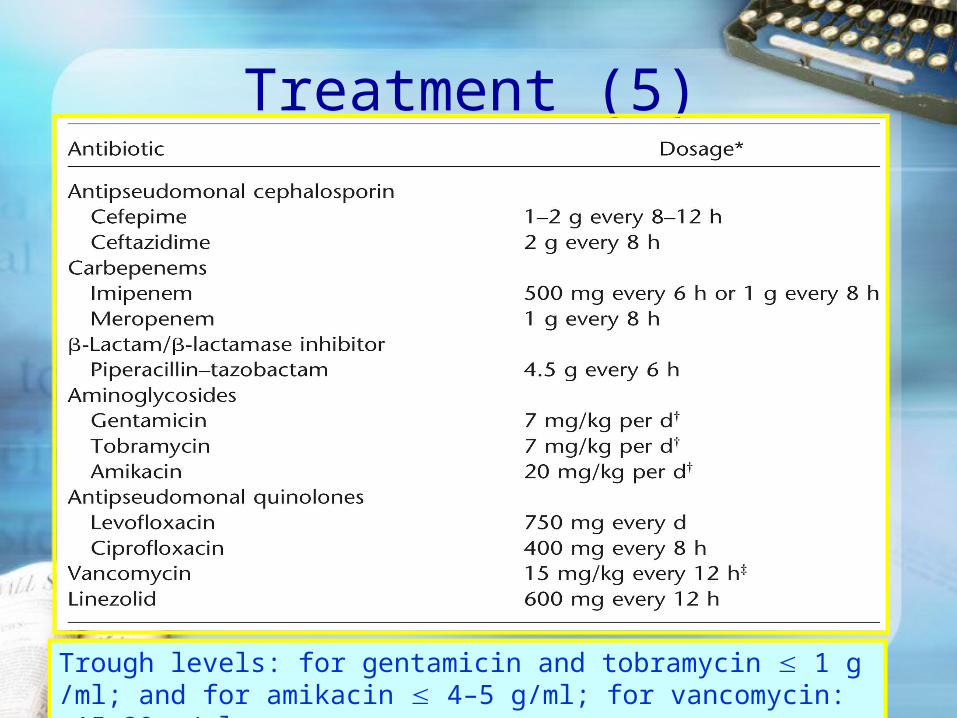
Treatment (5)
Trough levels: for gentamicin and tobramycin 1 g/ml; and for amikacin 4–5 g/ml; for vancomycin: 15–20 g/ml.
Treatment (6)Initial IV form; a switch to oral/enteral therapy;
Highly bioavailable agents, such as quinolones and linezolid, may be easily switched to oral therapy (Level II)
Aerosolized antibiotics have not been proven to have value in the therapy of VAP (Level I) However, they may be considered as adjunctive therapy in MDR gram-negatives pathogens, not responding to systemic therapy (Level III)
Treatment (7)Combination therapy: for possible MDR pathogens (Level II); No documented superiority compared with monotherapy, except to enhance likelihood of initially appropriate empiric (Level I)
Combination with aminoglycoside: stopped after 5–7 days in responding patients (Level III)
Monotherapy: Only in the absence of resistant pathogens (Level I)

Treatment (8)If initially appropriate ABx: efforts to shorten durati
on from the traditional 14~21 to 7 days, except P. aeruginosa, and with good clinical response & resolution of clinical features (Level I)
In P. aeruginosa pneumonia: combination recommended ( resistance on monotherapy); combination will not necessarily prevent the development of resistance, but avoid inappropriate and ineffective tx (Level II)
Treatment (9)In Acinetobacter species: the most active agents are the carbapenems, sulbactam, colistin, and polymyxin; no data documenting an improved outcome with combination regimen (Level II)
In ESBL Enterobacteriaceae: monotherapy with a third-generation cephalosporin should be avoided. The most active agents are carbapenems (Level II)
Treatment (10)Adjunctive inhaled aminoglycoside or polymyxin: should be considered for MDR gram-negative pneumonia, especially not improving with systemic therapy (Level III)
Linezolid: an alternative to vancomycin for MRSA (Level II), preferred in renal insufficiency or receiving other nephrotoxic agents, but more data are needed (Level III).
Treatment (11)Antibiotic restriction: limit epidemic infection with specific resistant pathogens Heterogeneity of antibiotic prescriptions: including formal antibiotic cycling
overall frequency of antibiotic resistance long-term impact of this practice: unknown
(Level II)

Response (1)Serial assessment of clinical parameters to define t
he response to initial empiric therapy (Level II)
Clinical improvement: takes 48–72 hours don’t change therapy during this time; unless rapid clinical decline (Level III)
Non-response: evident by Day 3, using an assessment of clinical parameters (Level II)

Response (2)

Response (3)In responding patient: de-escalation of antibiotics, narrowing therapy to the most focused regimen on the basis of culture data (Level II)
In nonresponding patient: evaluate for -noninfectious mimics of pneumonia
-drug-resistant organisms
-extrapulmonary sites of infection
-complications of pneumonia and its therapy. (Level III)



















